Electrocardiographic Markers of Ischemia and Scar
Coronary artery disease (CAD) describes complications that arise from a compromised blood flow to the cardiac muscle. Over time, deposits of cholesterol and fatty acids, calcium and other minerals form plaques attached to the inner lining of arteries. Plaque creates a rough, rigid surface that ultimately reduces the diameter of the intima of the coronaries, and elasticity of the vessel is lost (Atherosclerosis). In some conditions, plaques can become dislodged from the surface and become trapped in a distal region of an artery, causing a clot to form, ultimately starving the myocardium from its oxygen (blood) supply, causing infarction and tissue death.
Myocardial Ischemia is a condition whereby coronary circulation is insufficient to supply myocardial oxygen demands. A coronary spasm, occlusion by a thrombus or intracoronary plaque buildup may lead to partial or total starvation of oxygen rich blood to the heart muscle. Transient ischemia may occur with activity or at rest, and the victim may experience symptoms such as shortness of breath, back pain near the shoulder blades, jaw pain, chest tightness, dizziness, fatigue, or chest pressure. In the diabetic population, pain may not be reported at all.
Changes to myocardial tissue in the throes of an ischemic event lead to loss of tissue elasticity, wall motion abnormalities, and impaired function. The heart as a whole must work harder to compensate for these changes, and the left ventricle enlarges, there is reduced thickening during contraction, the heart rate increases, but the blood pressure and ejection fraction drop.
Development of myocardial ischemia depends on the location and severity of a stenosis, the presence or absence of collateral vessels, demands of the myocardium, and the coexistence of risk factors.
Clinical manifestations of myocardial ischemia include chest pain (angina pectoris) or other upper body discomfort due to reduction of oxygen delivery to cardiac muscle, myocardial infarction resulting from total arterial occlusion leading to cell death, and sudden death.
Impairment of Conduction
The coronary arteries also supply blood, oxygen and nutrients to the
heart’s conduction system. The consequences of impaired blood supply to the conduction system are variable:
- Blockage of posterior branch of the RCA will typically cause transient changes in the conduction system through the AV node.
- Impairment of circulation of the LAD usually results in a large myocardial infarction that may damage the bundle branches. Tissue death in bundle branches leads to permanent conduction delay. A heart block occurring at this level requires a permanent pacemaker- a device that stimulates contraction of the heart muscle by electrical impulses.
Ischemia Cascade and Stunning
With relatively increased flow demands or if there is an occlusion preventing adequate blood flow to the heart muscle, ischemia will result. The ISCHEMIA CASCADE begins with reduced perfusion, leading to diastolic and systolic dysfunction, ECG changes and pain. If oxygen demands are quickly reduced to baseline or if a complete coronary occlusion is quickly released, ischemia and its indicators are quickly reversed, and contractile function returns. ECG changes will return to baseline and chest pain and other symptoms will resolve. If perfusion is restored with some delay, contractile function may remain depressed, even for weeks. This causes “Stunning” of the myocardium.
Electrical Changes The 12-lead electrocardiogram, properly recorded over several days, demonstrates characteristic changes in over 75 percent of patients with myocardial infarction. Diagnosis is difficult to establish when an infarct is in an atypical location in the myocardium, the patient has had previous infarcts, the patient is receiving digitalis therapy, or when the electrocardiogram demonstrates a wide QRS complex. Usually, the ECG is used to confirm the clinical impression. It does not necessarily reflect infarct size,
give us any quantifiable data with respect to function (EF), nor can it indicate the prognosis.
As a rule, myocardial infarction produces distinctive electrical changes in the affected tissue. The area of dead tissue (infarct) is surrounded by a zone of injured tissue, which, in turn, is bordered by hypoxic tissue. Each tissue zone produces a characteristic electrocardiographic pattern, and each pattern undergoes characteristic changes as scarring and healing occur.
Prominent Q wave: Since dead tissue does not conduct electrical impulses, no current will flow toward an electrode that is placed directly over a necrotic area. Instead, an electrode so placed will record current flowing through the opposite ventricular wall in the opposite direction. Therefore, a negative Q wave or QS wave will be observed, as shown below.

Prominent Q waves indicate scarred myocardium.
Tissue death does not follow immediately upon obstruction of the vessel that supplied the affected area, so Q waves may not appear until several hours after the onset of pain. However, once the tissue is dead, it will not regain its capacity for conducting electricity. Therefore, Q waves generally remain visible over an injured area, although they may become smaller with the passage of years. Q waves resulting from myocardial infarction must not be confused with the small initial Q wave due to septal depolarization normally seen in many leads. To be significant, the Q wave must be wider than 0.03 second.
ST-segment elevation: Acute injury to the myocardium interferes with repolarization of the affected tissues. Transmural ischemia is characterized by elevation of the ST-segment over the affected area, as shown below. In acute myocardial infarction, reciprocal ST-segment depression is often seen in leads opposite the affected area. Following the acute period, the area of injury may die, or it may recover as a collateral blood supply is established. As the tissue recovers, the ST segment gradually returns to the normal position.
ST segment elevation
ST elevation vs depression
Hibernating Myocardium
Persistent flow reduction or repeated stunning may result in chronically depressed function. This induces “hibernation of the myocardium”. Irreversible damage leads to myocardial necrosis and eventual replacement of myocytes with dysfunctional scar. The LV dilates, thins, and loses elasticity, a process called “remodeling”. If this process is not reversed, the LV will continue to decline in function and heart failure will ensue.
Myocardial Infarction
Myocardial ischemia may produce inversion of T waves over the affected area. This inversion may return to normal when the attack subsides. T-wave inversion occurs in MI but may not be seen in acute stages. It may persist for years after the MI.

Inverted or “flipped” T-waves indicate myocardial damage
Transmural Myocardial Infarction
When the entire thickness of myocardial muscle is involved in this process, the result is a transmural infarction. Three characteristics of transmural myocardial infarction- Q waves, ST-segment elevation, and T-wave inversion- usually
occur in the following sequence:
ST-segment elevation is usually the first sign of acute injury.
Q waves begin to appear within a few hours to days, indicating death of myocardial tissue. By this time, the ST-segment has usually become lower, and inverted T waves are seen.
Several days or weeks after the infarction, Q waves can still be seen. The ST-segment has returned to baseline and T waves are symmetrical and inverted.
Years after the infarction, Q waves are usually still visible, but they may be smaller and the ST-segment and T wave may be normal.
Deadly Rhythms
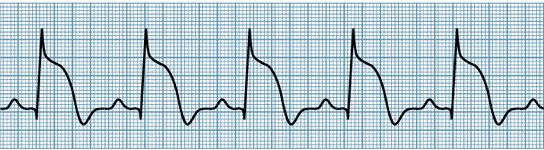
The pattern of Ventricular Tachycardia – the heart rate is over 100 beats per minute in at least 3 consecutive ventricular complexes.
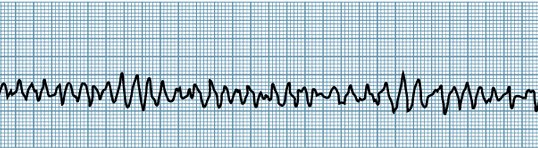
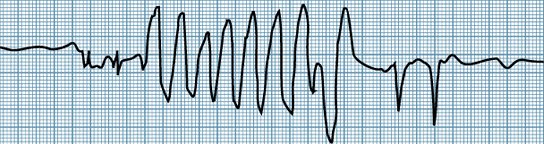
With Ventricular Fibrillation, there is no organized electrical activity at all. Symptoms include unconsciousness and no blood pressure. If this patient is not resuscitated and defibrillated right away, death will occur within 4 minutes.
Summing Up: ECG in MI
The three characteristics of transmural myocardial infarction—Q waves, ST-segment elevation, and T-wave inversion—usually occur in the following sequence:
1. ST-segment elevation is usually the first sign of acute injury.
2. Q waves begin to appear within a few hours to days, indicating death of myocardial tissue. By this time, the ST-segment has usually become lower, and inverted T waves are seen.
3. Several days or weeks after the infarction, Q waves can still be seen. The ST-segment has returned to baseline and T waves are symmetrical and inverted.
4. Years after the infarction, Q waves are usually still visible, but they may be smaller and the ST-segment and T wave may be normal.
These changes represent the expected evolution of myocardial infarction. Deviations from the usual sequence often indicate a complication. For example, ST-segment elevation that persists over a period of weeks may be a sign of ventricular aneurysm.