Identification of Arrhythmias
The normal electrocardiogram consists of a repetitive series of P, Q, R, S, and T waves which conform to established standards for size and shape and occur 60 to 100 times per minute. The term arrhythmia is used to describe any abnormality in the heartbeat, including disturbances in rate, rhythm, or conduction. Arrhythmias may be described as benign or lethal depending on the rhythm, the patient’s underlying condition, and the patient’s clinical response to the arrhythmia. For example, sinus tachycardia in a healthy person is usually of no clinical importance. Sinus tachycardia in a patient with a damaged heart, however, can result in life-threatening decreases in cardiac output.
Arrhythmias may occur constantly or intermittently. They can occur because of myocardial ischemia, drug toxicity, electrolyte imbalance, or overactivity of the sympathetic or parasympathetic nervous systems. Treatment of the arrhythmia depends primarily on the patient’s clinical response to the disturbance rather than the presence of the arrhythmia itself. In this slide show, you will see how abnormal ECG patterns differ from normal tracings. Furthermore, the etiology of the abnormalities will be presented. A firm understanding of ECG interpretation will enhance your ability to monitor a stress ECG study, identify arrhythmias prior to a radionuclide ventricular function study, and perform any nuclear cardiology procedure in the acute care or outpatient setting.
Arrhythmias can be identified on the ECG by following these steps:
Calculate the heart rate by counting the number of R waves in a 6-inch strip of ECG tracing (the equivalent of a 6-second time interval) and multiplying by 10 to get the rate per minute. Since the top margin of ECG paper is marked in 3-inch intervals, the heart rate can be easily calculated by this method. On the basis of heart rate, arrhythmias can be divided into three categories:
• Bradycardia: less than 60 beats per minute
• Normal rate: between 60 and 100 beats per minute
• Tachycardia: more than 100 beats per minute
Since several types of arrhythmias are characterized only by rate changes, these calculations are extremely important.
Note the regularity of R waves. When R waves occur at regular intervals (with a variance of less than 0.16 second per beat) the ventricular rhythm is regular. The ventricular rhythm is said to be irregular when there are differences in the duration of successive RR intervals. Dividing the ventricular rhythm into regular and irregular categories assists in identifying the mechanism of the arrhythmia.
Examine the P wave. If P waves are present and precede each QRS complex, the heartbeat originates in the sinus node and a sinus rhythm exists. The absence of P waves or an abnormality in their position with respect to the QRS complex indicates that the impulse starts outside the SA node and that an ectopic (displaced) pacemaker is in command.
Measure the PR interval. Normally, the PR interval is between 0.12 and 0.20 second in duration. Prolongation or reduction of this time indicates a defect in the conduction system between the atria and the ventricles.
Measure the QRS complex. If the duration between the onset of the Q wave and the completion of the S wave is
0.12 second or more (three fine lines on the ECG paper), an intraventricular conduction defect exists.
Normal sinus rhythm
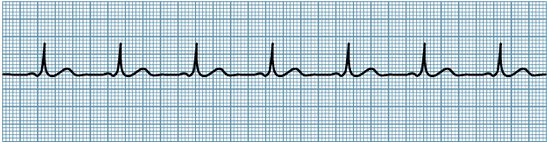
Rate: 60-100 beats per minute.
Rhythm: Regular.
P wave: Normal contour and precedes each QRS complex.
PR interval: Normal and constant (0.12-0.20 sec.).
QRS complex: Normal and constant (0.06-0.10 sec.).
The impulse originates in the SA node and travels through the AV node and ventricles in a normal fashion.
By following these steps, arrhythmias can
be categorized according to their origin and mechanism. Let’s evaluate
the ECG strips below.
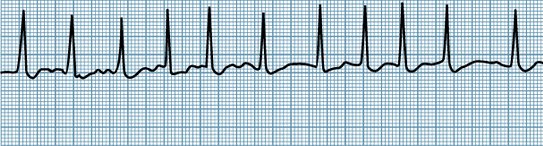
Sinus bradycardia

Rate: Below 60 beats per minute.
Rhythm: Regular.
P wave: Normal contour and precedes each QRS complex.
PR interval: Normal and constant.
QRS complex: Normal and constant.
Interpretation: The impulse originates in the SA node and follows the normal conduction pathways. Since the rate is below 60 beats per minute, this is a bradyarrhythmia. No medical treatment is necessary unless the rate is extremely slow and the patient becomes symptomatic (e.g., dizziness, hypotension, fainting). If treatment is necessary to increase heart rate, atropine is the drug of choice.
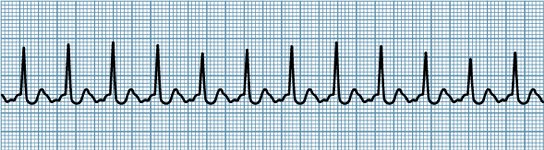
Sinus tachycardia
Rate: Above 100 beats per minute.
Rhythm: Regular.
P wave: Present and precedes each QRS complex. In very rapid rates, the P wave may be difficult to identify if it is buried within the preceding T wave.
PR interval: Normal and constant.
QRS complex: Normal duration.
Interpretation: The impulse originates in the SA node and follows normal conduction pathways. Since the rate is above 100 beats per minute, this is a tachyarrhythmia. In most individuals, stress, excitement, or exercise increases heart rate. Problems arise when this increased rate places a burden on a damaged heart. The goal of treatment is to lower the rate using drug therapy.
Sinus arrhythmia

Rate: May vary, but usually slower than normal.
Rhythm: Irregular.
P wave: Normal contour and precedes each QRS complex.
PR interval: Normal.
Interpretation: This rhythm is benign and requires no medical treatment. Phasic increases and decreases in heart rate are usually associated with inspiration and expiration, and are most noticeable during sleep.
Premature atrial contraction (PAC)
Rate: Normal, but may vary.
Rhythm: Regular, with the exception of PAC.
P wave: Normal P wave precedes each QRS complex, but the P wave associated with the premature beat may have a different configuration since it occurs outside the SA node. It doesn’t follow the normal atrial conduction pathways and may be hidden completely.
PR interval: PR interval associated with the early beat is usually longer than that of the sinus beat.
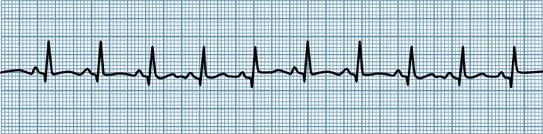
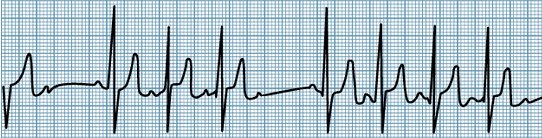
Atrial fibrillation
Rate: The atrial rate is usually above 350 beats per minute, and the ventricular rate is usually between 60 and 160, but may vary.
Rhythm: The RR distances are unequal. Therefore, an irregular ventricular rhythm is present.
P wave: Since no P waves can be identified, the sinus node is not the pacemaker. The existence of an ectopic pacemaker can be inferred.
PR interval: The PR interval cannot be measured since there are no P waves.
QRS complex: The QRS complex is 0.10 second and within normal limits. Therefore we may assume that conduction through the ventricles is normal and that the ectopic pacemaker is above the AV node.
Interpretation:
By definition, this is considered a supraventricular arrhythmia.
By combining all this information we can reason that the abnormality originates in the atrium, but not in the SA node. Because the ventricular beat is irregular, we may assume that the impulse does not arrive at the ventricles in a rhythmic fashion. The mechanism for this particular abnormality is fibrillation. The ECG interpretation is atrial (site) fibrillation (mechanism).
Using this approach to ECG analysis, let’s now look at some specific arrhythmias. When interpreting rhythm strips, remember to use all of these steps, as they are equally important.
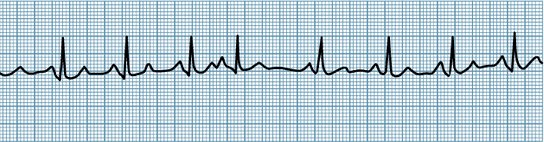
Atrial flutter
Rate: The atrial rate is in the range of 250–350 beats per minute, with the ventricular rate depending on the degree of AV block.
Rhythm: The atrial rhythm is regular, and the ventricular rate may be either regular or irregular.
P wave: P waves are replaced by “f” (fibrillation) waves and identified by undulations of varying contour, amplitude, and spacing.
PR interval: Unable to measure.
QRS complex: Usually Normal.
Interpretation:
When impulses are discharging in the atria at such rapid rates, the normally slower rate of conduction through the AV node acts as a filter to block some of the impulses from reaching the ventricles. When the ventricles respond only to every other atrial impulse, it is defined as atrial flutter with 2:1 AV block. Ventricular response to every third impulse would result in a 3:1 AV block. In the latter case, the atrial rate would be 300 and the ventricular rate would be 100. The patient may be asymptomatic or may describe a fluttering sensation or palpitation. Treatment is the same as that for atrial fibrillation, with synchronous DC conversion employed when the patient is compromised hemodynamically. Signs of poor cardiac output include oliguria, hypotension, diaphoresis, and change in mental status.
Supraventricular Tachycardia

Rate: 150–250 beats per minute.
Rhythm: Regular, except at onset and termination.
P wave: Difficult to identify, since it is often superimposed on the preceding T wave or hidden within the QRS complex.
PR interval: Usually constant if the P waves can be identified.
QRS complex: May be normal or widened if an aberrant conduction is present.
Interpretation:
Supraventricular tachycardia is the term used to describe any tachycardia that occurs above the ventricles. This includes paroxysmal atrial tachycardia (PAT) and paroxysmal junctional tachycardia (PJT). Because the rapid rates can obscure the P waves, making it impossible to determine the origin of the impulse, the rhythm is termed SVT. Both PAT and PJT are characterized by rapid, regular, atrial or junctional tachycardias of sudden onset and termination, with rates of 150–250 beats per minute. Clinical presentation, ECG characteristics and treatment for both conditions are virtually the same. The rhythm usually begins with a premature atrial or junctional beat.
This arrhythmia can occur at any age and may or may not be associated with coronary artery disease. It can occur as a result of stress or excessive caffeine or nicotine intake. The patient may be asymptomatic, or may complain of angina-like pain, palpitations, or anxiety, depending on the duration and rate of the rhythm. Because of the rapid ventricular rate, SVT may cause reduced cardiac output, decreased cerebral perfusion, or syncope.
First-degree AV Block
Rate: Normal.
Rhythm: Regular.
P wave: Normal contour and precedes each QRS complex
PR interval: Prolonged (greater than 0.20 second).
QRS complex: Normal duration.
Interpretation:
The impulse originates in the SA node but is abnormally delayed as it travels through the AV node or bundle of His. Once the impulse passes the AV junctional region, it propagates normally through the ventricles. The ECG abnormality is demonstrated by the prolonged PR interval. This delay may be due to ischemia of the AV node or may be drug induced (e.g., lidocaine, digitalis, quinidine, or procainamide). If the arrhythmia is drug-induced, the physician should be notified and the patient’s drug regimen reassessed.
Second-degree AV Block (Wenckebach Mobitz Type I)

Rate: The atrial rate is normal. However, the ventricular rate is slower than the atrial rate because each atrial impulse does not always trigger a ventricular response.
Rhythm: The atrial rate is regular, but the ventricular rate is irregular.
P wave: Normal, but may be hidden in the preceding T wave as the PR interval lengthens.
PR interval: Progressively lengthens until a nonconducted P wave occurs.
QRS complex: Normal in duration.
Interpretation:
In this arrhythmia, impulses from the SA node are progressively delayed as they travel through the AV node or bundle of His until one impulse is completely blocked. There is a P wave, but no subsequent QRS complex. The cycle is then repeated. This is a more advanced degree of block that is sometimes seen in acute inferior MI due to ischemia of the AV node. The physician should be notified.
Second-degree AV Block (Mobitz Type II)
Rate: The atrial rate is normal, but the ventricular rate is slower.
Rhythm: The atrial rhythm is regular, but the ventricular rhythm is irregular.
P wave: Normal, but not always followed by a QRS complex.
PR interval: May be normal or slightly prolonged but remains constant, except for nonconducted P waves.
QRS complex: Usually widened, since a bundle branch block is frequently present.
Interpretation:
In Mobitz Type II, the atria are stimulated normally by the SA node. Not all of the impulses, however, are conducted through the AV node and bundle of His to stimulate the ventricles. The patient may be asymptomatic or may show signs of decompensation, depending on the ventricular response. If the patient is tolerating the rate well and not showing any clinical signs of decompensation, then the only acute treatment may consist of continued monitoring.
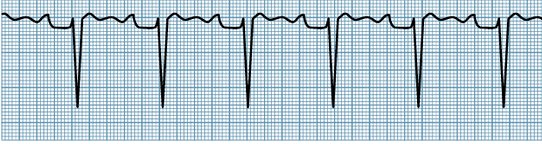
Third-degree AV Block with Ventricular Pacemaker

Rate: The atrial rate is faster than the ventricular rate.
Rhythm: The atrial and ventricular rates are regular but independent of each other.
P wave: Normal contour, but no fixed relationship to the QRS complex.
PR interval: Constantly changing.
QRS complex: The configuration depends on the site of impulse formation. If the impulse arises high enough in the conduction system, the QRS is fairly normal. If it originates in the ventricles, however, it is wide and aberrant.
Interpretation:
Despite normal impulse initiation in the SA node and depolarization of the atria, no impulses are transmitted to the ventricles. Because the ventricles are not receiving any stimulation, a subsidiary pacemaker assumes the role of impulse initiation for the ventricles. Therefore, the atria and the ventricles each have their own pacemaker with their own rates and are stimulated and contract independently of each other.
Premature Ventricular Contraction
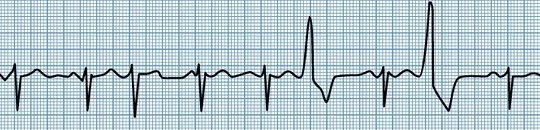
Rate: Usually normal.
Rhythm: Regular, except when interrupted by the premature beat.
P wave: Normal contour, and precedes each QRS complex except with the premature beat, when there is no P wave.
PR interval: Constantly changing.
QRS complex: Normal, except with the premature beat, when the QRS is wide and bizarre, with the T wave usually opposite in direction to the QRS complex.
Interpretation:
PVCs occur because one or more ventricular foci discharge prematurely, causing a ventricular contraction. Because the impulse originates in the ventricle and does not follow the normal pathway of conduction, the resulting QRS complex is wide and bizarre. There is no P wave preceding the premature beat because there is no atrial stimulation.
Some PVCs are benign, resulting from cigarette smoking, caffeine intake, lack of sleep, or emotional stress. PVCs also may be caused by pathological conditions such as ischemia or hypokalemia. Because PVCs occur before the ventricle has filled completely, the stroke volume of the resulting contraction is less than normal. If PVCs are numerous, they may burden a damaged heart. The patient may complain of a thumping, fluttering, or skipping sensation in the chest or may be symptom-free.
PVCs are usually treated in acute MI patients if they occur more often than five per minute, if there is a run of two or more together, or if they are multiformed, as evidenced by PVCs having at least two different configurations. Multiform PVCs may indicate that the PVCs are coming from more than one irritable area in the ventricle. Treatment is also necessary if PVCs occur during the preceding T wave, which is the vulnerable period during which ventricular tachycardia is more likely to occur.
DEADLY RHYTHMS
Ventricular Tachycardia
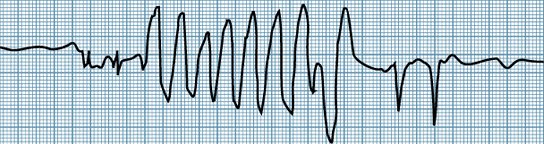
Rate: The ventricular rate is usually 120–200 beats per minute.
Rhythm: Regular or slightly irregular.
P wave: Usually obscured by QRS complexes, but may be inverted (opposite of sinus rhythm) and not associated with the ventricular rhythm.
PR interval: Not able to determine.
QRS complex: Widened beyond 0.12 second. It has a bizarre configuration, with the T wave usually opposite in direction to the QRS complex.
Interpretation:
Ventricular tachycardia is defined as a series of three or more consecutive ventricular complexes. It may last seconds, hours, or days. In most cases the rate is too fast to provide an adequate cardiac output. Mental confusion, convulsions, or unconsciousness will reflect a decreased blood flow and oxygen supply to the brain. Immediate treatment is necessary if any of these symptoms occur. DC cardioversion is the treatment of choice if the patient is hemodynamically unstable. Otherwise, intravenous lidocaine, procainamide, or bretylium can be used.
Ventricular Fibrillation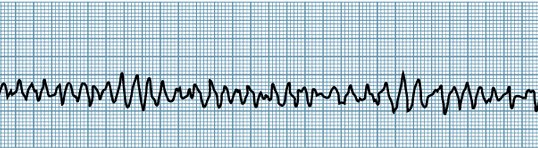
Rate: The ventricular rate is greater than 300 beats per minute.
Rhythm: Grossly irregular.
P wave: Unable to measure.
PR interval: Unable to measure.
QRS complex: Replaced by undulations of varying contour, amplitude, and spacing.
Interpretation: The lack of synchronous ventricular activity results in an ineffective ventricular contraction. Because the ventricles are merely quivering rather than contracting, there is no effective cardiac output. Thus, loss of consciousness, convulsions, and death occur rapidly unless treatment is instituted immediately. DC cardioversion with cardiopulmonary resuscitation (CPR) employed between countershocks to maintain circulation is the only effective treatment of ventricular fibrillation.